Ever looked at a patient’s EKG and thought “I wonder if this is Atrial Fibrillation?” Obviously not, you’d say A-fib cause you’re not a nerd. But the point remains. What rhythm is my patient in and what am I going to do about it?
Time to break down everything you need to know about abnormal atrial rhythms. Specifically Atrial Fibrillation, Atrial Flutter, and Premature Atrial Complexes (PAC’s). Let’s have a look.
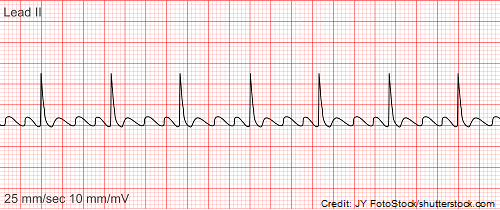
I’m assuming you already know what a normal ECG looks like, and you can pretty easily tell where your P-waves are at. But look at this one

R- R intervals are irregular. R waves are narrow and not slow enough to be ventricular. What’s happening between the R waves, though? Initially we could say it’s A-fib but you could also argue for it being PACs with a bunch of artifact. How do you tell?
The biggest thing ruling out artifact is the isoelectric line – the flat line on your EKG- being relatively consistent across the entire strip. If we saw any significant deviation in level I might be more concerned about it being artifact. Pretty sure the EKG below means your driver just hit a speed bump at 30 MPH in the box.
Now we can take a closer look at what’s going on between our R waves in the first strip. The deviations from the isoelectric line look pretty similar in morphology but if you look closely you can see some differences in width and amplitude. They are also not firing at regular intervals. This means that we have multiple locations that are firing off giving us this electrical deviation i.e. multiple foci.
They also are definitely not our QRS complex so we can rule that out, and we have a visible T wave which looks nothing like what we’re seeing between complexes. We are left with the possibility these are many different atrial cells rapidly depolarizing.
So we have rapid, multifocal atrial depolarizations which are not correlated to a QRS complex meaning…A-fib for sure. Turns out you were right the first try. Congrats.
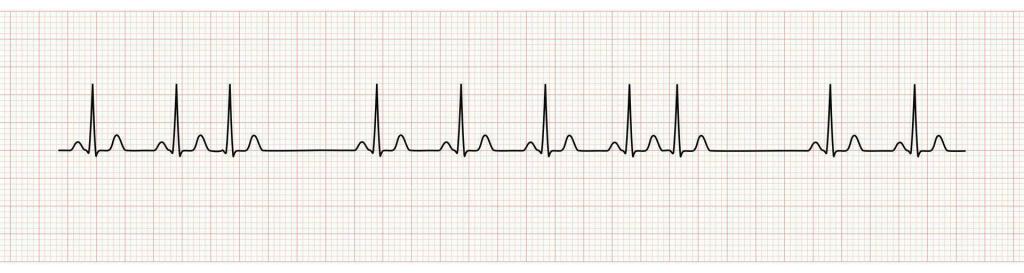
Neat heart block huh? Nope this is a sinus rhythm with PACs. Notice there is no distinct P wave on our irregular beats. That won’t always be the case but here its just running into the preceding T wave.
PACs can be difficult to diagnose because the R-R intervals are technically irregularly irregular, a tell-tale sign of A-fib. But we don’t have the constant depolarization of the atrial cells. What we are actually seeing is just a random extra depolarization of a pacemaker cell that makes it to the AV node and fires the ventricles.
After that extra beat we see a compensatory pause. This can throw you off if you’re too quick to judge. It looks like a dropped beat from a type 2 heart block. What’s actually happening is the heart realizes it didn’t need that extra contraction and takes a momentary nap to set itself right again. We don’t see these too often in the field, probably because we aren’t doing enough to look for them.
Alright last bit, A Flutter.
In my mind these are the easiest to indentify. We still have a regular R-R interval across the strip so it’s neither A-fib nor a PAC. The QRS is narrow so it’s not Junctional or Ventricular. Sinus rhythm it is. But the atrial cell firing off is going a million miles a minute due to a reentry circuit. It triggers over and over and over with only some of those signals making it through to the ventricles at regular intervals. Congrats the AV node is doing it’s job today.
The morphology of these P waves is consistent across the board meaning the depolarization is coming from a single pacemaker cell in the atria. A flutter is quick to diagnose on scene. Those smooth rolling hills stand out better than a STEMI.
What does all this have to do with how we treat these patients? Not much. Going off of nothing more than these strips there isn’t really anything we should do. Heck if they’re stable I may forgo an IV and send them BLS. None of these rhythms are an emergency in and of themselves. Who knows how long 70 year old Mrs. Johnson has been in A-Fib? I’m not about to do anything about it. Fluids may help your A-fib or PAC patient but again, if they’re stable why are you poking about? If it ain’t broke don’t fix it.
There’s tons more to say about atrial rhythms but this is enough for today. See you next time!
And if you want to learn more about us go HERE

And if you’re looking for a little more help, I partnered with Pocket Prep.
It’s something we give to all our students. In fact, we include it with their class. It’s that useful. Every course we get tons of students telling us how helpful it was in passing the class.

Leave a comment